Minimally invasive surgery
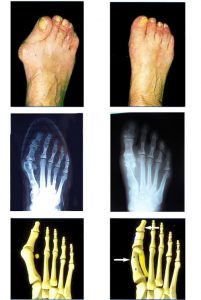
Surgical correction of deformations
The principle is not limited to “planning” the bunion (consequence of deformation), but to addressing the cause. From now on, all interventions acting only on the soft parts (tendons, joints) have been abandoned. It will be necessary to realign the big toe to allow the shoes ’s wearing, and re-harmonize the arch, so that during the natural way of walking, the forefoot uses the whole plantar surface to propel itself forward.
The surgical incision is located on the inner edge of the foot. We will first release the soft tissues and the joint by severing the side fasteners, and perform an exostosectomy (planning the bunion).
Then we will bring the first metatarsal back in parallel position to the second. To do so, we will have to straighten it out. This is achieved through SCARF-type translation osteotomy (or bone cut). The first metatarsal is cleaved or split in 2 parts, so as to slide it towards the second metatarsal. The 2 bone fragments will be fixed by nesting (without metallic material).
If a deformation persists, we can complete it with a gesture on the first phalange.
At the end of the procedure, the associated claw toes will be supported, or the lateral metatarsals will be shortened, if the procedure results in an imbalance of the plantar arch.
The foot will be less wide by one centimeter, and the size of the foot will remain unchanged
The scar: you will have only one scar (which will become very thin after a few months), along the inner edge of the foot. It will be approximately 35 to 40 mm in term.
This is a minimally invasive surgery. It responds at the same time to an aesthetic concern, to a simplification of the operating suites and to a reduction of the functional recovery time.
Complications of the surgical procedure
Phlebitis and Pulmonary Embolism (clot in veins that can migrate into the pulmonary circulation). Normally you will walk from the night of the surgery, so this is a low risk. If you have a history or risk factors, anticoagulant treatment may be prescribed, depending on the patient.
Stiffness. Against this we recommend a self-rehabilitation explained in the chapter «post-operative care», which allows to carry out rehabilitation several times a day, and every day. If at 45 days there is a lack of mobility, physiotherapy sessions will be prescribed.
Recurrence. Recurrence occurs only if the angle between the first and second metatarsal bone is not sufficiently reduced. It is nevertheless necessary to avoid risky behaviors like the practice of classical dance with realization of spikes, climbing. Similarly, it is not advisable to wear heels too high, too long and too often.
Hallux Varus. It is an excess of correction, the big toe going back too far inside. This creates a crippling discomfort when riding.
Infection. At the foot clinic, we prefer techniques without equipment. Therefore, there is no metallic foreign material, thus reducing the infectious risk
Scarring delay, and hematoma from the surgical site.
Consolidation delay. In this case the shoe to support heel longer.
Algoneurodystrophy. Feared complication with type of violent pain related to neuro-vascular problems. It lasts 12 to 18 months, and occurs for no identifiable reason. The risk will decrease with the administration of Vitamin C for one month. If it arrives, after confirmation by a nuclear exam, and requires to consult a Pain Clinic.
Edema (swelling of the operated area). It can last between two and three months. This is inevitable whatever the surgical technique chosen. It is not strictly speaking a complication, this is logical and usual. It will depend on your application to raise the foot and frost it to prevent it as much as possible.
Exceptional risks: Toe necrosis (vascular injury), Metatarsal bone assembly disassembly (spontaneous or post-traumatical), Loss of sensibility (neurologic injury)


